






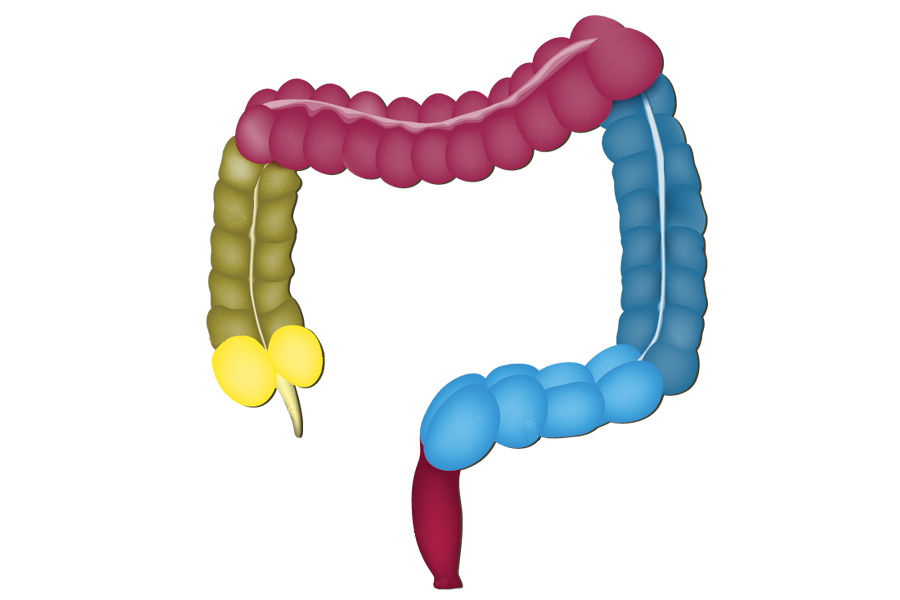
What is a colostomy? Well, first, take a look at the diagram below – quite intricate!

Acids and enzymes turn food into a liquid mixture when inside the stomach. From here, the liquid mixture is passed into the small intestine, where digestion takes place. Anything that is not absorbed by the body during the digestion process is considered waste and later eliminated.
We’re familiar with the “natural” methods of elimination, however, individuals who have been struck with illnesses and diseases (more below) that hinder these bodily functions must find alternate ways for waste to leave the body. Enter: ostomy.
An ostomy is a surgical procedure that creates a new opening for the passage of feces, urine or both. Though there are several types of ostomy procedures (colostomy, ileostomy, urostomy), today’s focus will be on understanding a colostomy.
During a colostomy, one end of the colon (aka large intestine or bowel) is pulled out through the abdomen then connected surgically to the outer surface of the abdominal wall to construct a stoma, which allows for the discharge of feces. Waste, which can be anywhere from runny to firm, will now drain from the stoma into a pouch that is adhered securely to the skin.
The location and size of the stoma will differ based on diagnosis and which part of the colon (ascending, tranverse, descending or sigmoid) is used to create it. All healthy stomas should be red and moist (much like the inside of a person’s mouth). Since there are no nerve endings, stomas are not painful and bleeding usually only occurs if irritated or rubbed accidentally.
Though the list of reasons for a colostomy may be extensive, some of the common conditions include:
- Colorectal Cancer: rising from the lining of the colon and rectum
- Ulcerative Colitis: inflammatory bowel disease that strikes in the colon.
- Diverticulitis: pouches form in the wall of the colon resulting in inflammation or infection.
- Hirchsprung Disease: a developmental disorder of the nervous system, characterized by an absence of large nerve cells in the distal colon that result in obstruction.
- Partial or complete blockage of the large bowel (intestinal obstruction)
- Wounds or fistulas in the perineum
- Trauma or injury to the affected area
Not all stomas are forever. In fact, colostomy reversals are quite common nowadays; the overall unique condition of a patient will dictate the permanency (or not) of their situation.
Colostomates work very closely with their doctor or ostomy nurse to learn how to manage their lifestyle, especially soon after the procedure. Proper use of a wide array of products (such as pouches, skin barriers, stoma measuring guides and many other items) along with following a healthy diet and exercise program, are important elements of a colostomate’s daily routine. All that, in combination with a positive frame of mind, can help ensure maximum quality of life for many, many years.
Sources: United Ostomy Associations of America, Inc., www.ostomy.org, Prevent Cancer Foundation
This article was written by a contributing author at Shield HealthCare.














I have had my colostomy since I was 11, I am 36 now. I am having trouble getting stuff to pass through the stoma. I have tried everything that I can think of but nothing seems to help. Can you please give me some ideas? It would be greatly appreciated. Thank you for your time.
Jacki Hale