By Peter Frost and Marcia Frellick, Chicago Tribune | April 26, 2014
Sherry Loveless can see the promise of managed care right through her bedroom door.
Saddled with multiple disabilities, Loveless, 61, has been stuck in her Rockford bedroom for months because the doorway is too narrow for her wheelchair to squeeze through. When she moved into the house in December, firefighters carried her to the bed.
But next month, thanks to a restructuring in Illinois’ Medicaid program, a renovation project is scheduled to widen the door and build a ramp that will allow her access to the outside.
The nonprofit that’s now in charge of Loveless’ health and well-being, Community Care Alliance of Illinois, also is making it easier for her to obtain medications for her arthritis, hypertension, diabetes and chronic obstructive pulmonary disease, as well as transportation to medical appointments.
The idea is that by investing upfront in Loveless’ quality of life and better managing her ailments, she’ll be healthier in the long run and save both the company and the government money.
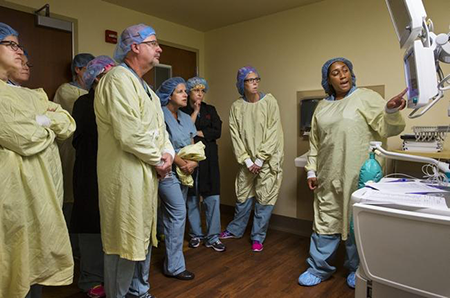
While most patients won’t get this degree of personal attention, hundreds of thousands of Medicaid recipients in Illinois are being shifted into some kind of managed care this year as part of a sweeping overhaul intended to fix a program widely acknowledged to be broken.
Medicaid traditionally reimburses hospitals, physicians and other providers for each service they perform, a system that rewards volume instead of quality. Now many will receive a fixed monthly payment for each patient they supervise, allowing them to profit if they keep people healthy.
The shift will change the way patients interact with the health care system, which in the past largely left people to fend for themselves and often resulted in substandard care and expensive hospital visits.
And by following other states into a managed care model, Illinois has a chance to reduce waste and duplication in its $15 billion Medicaid program, which consumes a large portion of the state’s cash-strapped budget.
“I’d consider this to be the most significant redesign of the Medicaid program in its history,” said Julie Hamos, director of the Illinois Department of Healthcare and Family Services, who called care coordination key to solving many of the program’s major problems.
Under state law, at least half of Illinois’ roughly 3 million Medicaid recipients must move into managed care programs by Jan. 1, including an estimated 350,000 who are expected to gain coverage this year under an expansion of eligibility allowed by theAffordable Care Act.
Managed care, Hamos said, “is the direction that the whole world is going” and, if done right, will produce “healthier people, lower costs and a more efficient delivery system.”
To participate in a managed care program in Illinois, a health plan must provide a vast range of services, including hospitalization, primary care, specialty care and mental health services. In exchange for this greater access, patients must accept limits on which doctors and hospitals they can visit.
But some also will receive perks like unlimited prescription drugs, free transportation, financial counseling, cellphones to call doctors and care coordinators, even gift cards for seeking preventive care.
Because health care providers have more of a financial stake in their patients’ well-being, some people — particularly those with chronic or multiple health conditions — can expect physicians and other employees to become more involved in their daily lives.
Care coordinators will be checking whether patients take their medications and attend medical appointments. They’ll be conducting more in-home visits. In Loveless’ case, Community Care Alliance hopes that putting about $6,000 into her home renovation will pay off in lower health care costs over the long term.
The cost “is less than the cost of one month of nursing home placement for an individual, which is really what (Loveless’) alternative option is,” said Anne Downs, a coordinator working with the Rockford woman. “By making this investment upfront, we’re saving money in the long run and the enrollee is safer.”
For Loveless, the project offers a small amount of independence that she’s coveted for months. Her goals are simple: She wants to join her congregation on Sundays instead of speaking with church leaders by phone. She wants to visit a store, something she says she hasn’t done in nearly eight years. Above all, she just wants to go outside.
“I think I’ll just sit for a while and look across the street,” she said.
The shift to managed care will take various shapes in Illinois, with different health plans for disparate parts of the Medicaid population. Some plans will be run by insurers likeAetna, Blue Cross and Blue Shield of Illinois and Humana; others will be run by networks of hospitals and health systems.
The transformation amounts to a giant transfer of financial risk from the government to insurance companies and health care providers. In exchange for assuming that risk, those companies get to keep a portion of any savings they’re able to generate by keeping patients healthier and out of the hospital.
Still, the margins are narrow, and there’s no guarantee of a profit. Under state contracts, health plans must spend at least 88 percent of the funds they receive on health care and related services; unspent money must be returned to the state. Profits come from the remaining 12 percent, after overhead costs are covered.
If a health plan’s costs exceed payments from the state, it must absorb the loss, not taxpayers.